
How the 21st Century Cures Act Changes Your EHR Integration Requirements
In 2026, interoperability has strongly shifted from just a technical requirement to a compliance requirement. With the enforcement of the 21st Century Cures Act in September of 2025, this changed how hospitals accessed, shared, and integrated patient data. Most importantly, especially for healthcare CTOs, it has almost rewritten or, more precisely, solidified the importance of interoperability. Although the 21st Century Cures Act is not new, its rules were enforced in phases by CMS (Centers for Medicare and Medicaid Services) and ONC (Office of the National Coordinator for Health Information Technology), and have solidified the core rules, such as information blocking prevention and developing API-first, patient-centric systems. These changes are directly reshaping how EHRs are designed. For instance, the legacy systems that used a custom HL7 interface must upgrade to FHIR-based APIs for seamless data sharing and meeting regulatory requirements. At the same time, the 21st Century Cures Act EHR requirements now need expanded access to Electronic Health Information (EHI) with real-time access to all patients without restrictions across systems and applications. That’s why it’s now important to understand the changed requirements before designing your EHR. In this blog, we will break down the EHR integration requirements under the 21st Century Cures Act, along with strategies to meet these patient data access rules while building a future-proof healthcare system.
The Core Shift: EHR Integration Requirements Under the Cures Act
After the enforcement of the 21st Century Cures Act compliance, interoperability transformed from a strategic investment to a compliance requirement. At first, interoperability was for only making data exchange smoother or adopting value-based care models.
But today, that thinking is no longer viable as new regulations under ONC and CMS require systems to allow seamless access to all Electronic Health Information (EHI). This means patients and health applications must be able to access, exchange, and use health data without any unnecessary limitations. And if you fail to comply with this, then it can be considered information blocking, leading to heavy penalties up to $1 million dollars.
Moreover, the scope of what information an EHI includes has also increased. Now, healthcare organizations also have to share nearly everything from clinical notes and lab results to medications and care plans.
However, adapting to this shift requires systems that support real-time data exchange and granular data access. This is what changes the whole architecture of EHR systems as they require standardized frameworks such as FHIR APIs.
In short, just connecting systems is no longer enough; now EHR integration must be compliant, standardized, and real-time.
EHR Interoperability Compliance Readiness Checklist (2026 Edition)
Get NowStandardized API Access & Technical Evolution
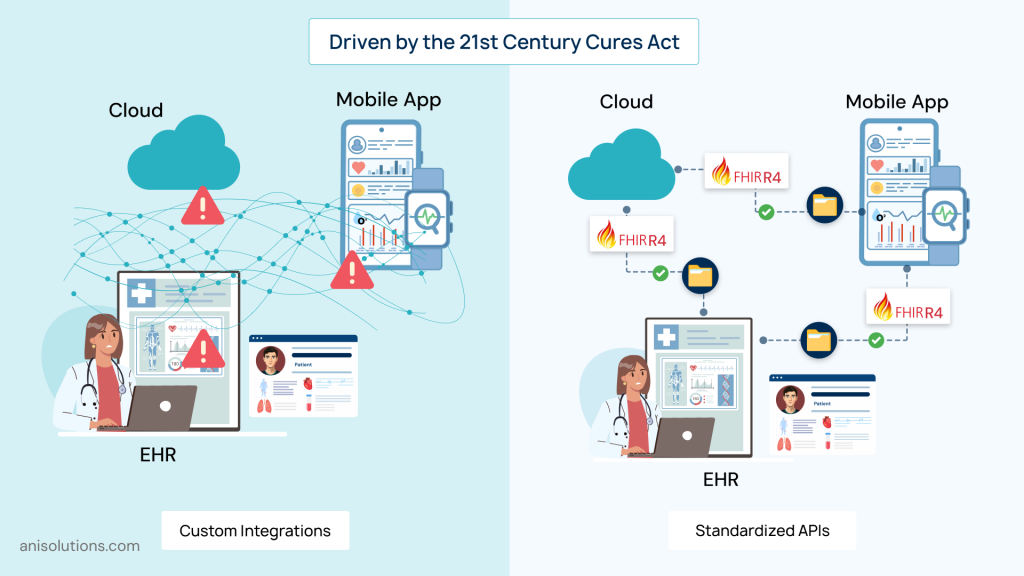
The Cures Act’s impact on healthcare data exchange has been significant, as the way EHR integration works has transformed completely. It is moving from its point-to-point integration to standardized APIs.
Before, the healthcare organizations used custom HL7 interfaces to connect each new connection added to the system. While this worked, these interfaces supported only specific workflows. Most importantly, they were difficult to scale and expensive to maintain, along with providing very limited flexibility for system expansions.
Now, all healthcare providers must have standardized API access for EHR systems under the Cures Act. And this is where FHIR comes in, matching the structure and format of patient data to the new healthcare data interoperability regulations.
Here, you need to build on the baseline required by the ONC health IT certification, which is the R4 (Release 4). This provides stable data modes for patients, observations, etc. Along with that, it also includes RESTful API structure and SMART on FHIR compatibility for effortlessly connecting with third-party applications.
With FHIR and R4 structure, you don’t need to build custom workflows for each system, building a scalable and reusable integration model. But this is not the only change, and healthcare organizations must adapt to USCDI v3 as well, to set a baseline for the types of data to access, including clinical documentation and social determinants of health (SDOH).
This enforcement of the 21st Century Cures Act compliance also requires healthcare systems to connect with third-party applications, from patient health apps to digital health platforms. So, the healthcare systems must have API-first architectures, where interoperability is built at the core and not outside the system, ensuring compliance, scalability, and long-term adaptability.
Patient Data Access Rules & Their Impact
One of the most transformative changes that the 21st Century Cures Act has brought is in patient data access rules. It has completely placed the control of what data they want to share and access into patients’ hands.
Previously, patients had to access data from the healthcare provider’s portal or request the patient records manually. But now, not only do they not have to request the data, but they can also view it through any third-party application of their choice.
This happened with the complete implementation of information blocking rules, which require organizations to share timely and seamless access to EHI. And this EHI is not just summaries of clinical data but complete datasets of clinical notes, lab reports, medications, and care plans.
However, this also means that systems have to build their architecture on standardized, API-based interactions. This also helps in completing the real-time availability requirements for both patients and regulatory bodies, such as the CMS and the ONC health IT certification. So, the systems must support automated data exchange instead of batch-based or manual procedures.
Although the data access has become patient-first, healthcare organizations need to ensure it is exchanged in a secure, authorized, and compliant manner, even through third-party applications.
In short, EHR integration is no longer just a system-to-system connection but a broader ecosystem where open patient access, connectivity, and regulatory compliance are interconnected.
FHIR R4 Implementation & API Strategy Blueprint
Download NowKey Compliance Requirements for Healthcare Organizations
As integration regulations evolve, compliance is no longer tied to a single mandate. Healthcare organizations must now align with overlapping regulatory requirements driven by the 21st Century Cures Act, CMS, and the ONC.
These regulations collectively define how Electronic Health Information (EHI) must be accessed, exchanged, and secured. For healthcare IT leaders, the challenge is not just understanding these requirements but translating them into practical architectural decisions that ensure long-term compliance and scalability.
Here is a table that outlines the core 21st Century Cures Act EHR requirements, along with their direct impact on EHR integration strategy and system design:
| Requirement Area | What the Rule Requires | Architectural Impact |
| Information Blocking Prevention | EHI must be accessible, exchangeable, and usable unless a valid exception applies | Requires open data access layers, audit logging, and rule-based access controls |
| Standardized API Access | Systems must provide API access “without special effort.” | Mandates FHIR-based API architecture with scalable, secure endpoints |
| EHI Scope Expansion | Nearly all patient data must be available for access and exchange | Requires unified data models and support for structured + unstructured data |
| Patient Data Access Rules | Patients can access their data via third-party applications | Requires external app integration, consent management, and identity controls |
| ONC Health IT Certification | Systems must meet interoperability and API compliance criteria | Requires conformance testing, validation environments, and reporting mechanisms |
| Transparency Requirements (DSI) | Clinical decision support and AI logic must be explainable | Requires model transparency, traceability, and auditability layers |
| HTI-1 Compliance (2026) | Expands interoperability and transparency mandates | Requires future-ready architecture aligned with evolving regulatory updates |
Challenges in Meeting Cures Act Requirements
While it sounds good to have a clear expectation for interoperability and data access, implementing these requirements in the organization comes with significant challenges.
The first challenge is to modernize the custom HL7 interfaces and integration points to match the API-based interoperability. These systems were not designed to exchange real-time data sets efficiently. And to transition them to FHIR-based APIs, healthcare organizations need complex data mapping, heavy transformation layers, and a redesign of architecture.
Additionally, even if the data is exchanged seamlessly, the systems require understanding it, and here the next challenge is. Building systems with semantic consistency is difficult if the systems operate without a clear understanding of different formats, coding standards, and clinical contexts, which can lead to inconsistent and inaccurate patient records.
One more challenge that organizations face is maintaining security and open access at the same time. The patient data becomes patient-first and free to access, but its security, privacy, and compliance must be maintained by the providers through authorization and authentication.
Then the next challenge is managing vendor alignment with all the connected applications and systems. Each vendor has different technologies and supports different standardization frameworks, and if they are not connected compatibly, it leads to fragmentation and inconsistent interoperability capabilities.
Most importantly, as healthcare is becoming more AI-driven and with the transparency requirements, healthcare organizations must ensure that each AI insight is explainable, traceable, and compliant.
Patient Data Access & App Integration Framework (Cures Act Ready)
Click HereA Strategic Approach to Cures Act-Compliant Integration
To solve the challenges mentioned in the point above and meet all the regulatory requirements, you need a structured strategy.
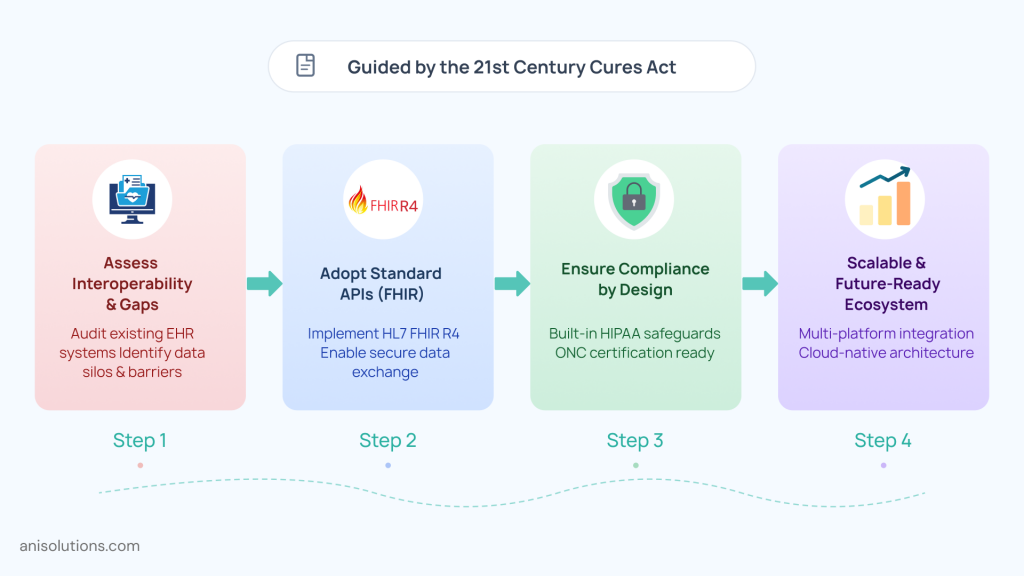
The first step in this process is to assess your current interoperability and its maturity. You need to identify the level of interoperability and how well it supports EHR access, along with identifying gaps in API readiness. While doing this, see where the existing workflow structure can lead to information blocking, technically or intentionally. This gives you a foundation to build improvements for the system.
The second step is to carefully transition toward API-first architecture using the identified gaps for reducing the operational and compliance risks. In modern healthcare, the systems must be able to exchange data through standardized APIs based on FHIR. This architecture allows you to build scalable, reusable, and consistent data exchange across platforms.
While all this is important, maintaining compliance is also equally important, and you can achieve it by aligning your long-term interoperability goals with compliance. The best way to approach is by building the compliance into the interoperability and system architecture. This ensures that compliance is not compromised along with operational efficiency, innovation, and ecosystem connectivity.
Finally, interoperability must be built for long-term scalability and adaptability as regulatory requirements are continuously changing. Moreover, the data requirements are also expanding over time, and your systems must be able to adapt to them without rebuilding with each new expansion or update.
In short, you need to adopt an API-based and future-ready approach to build interoperable systems that are scalable and aligned with the evolving healthcare landscape.
Conclusion: From Compliance to Competitive Advantage
In a nutshell, the 21st Century Cures Act is building true interoperability in healthcare organizations. Although with these changes, the healthcare organizations will face some challenges in redesigning their legacy systems, those who adopt quickly will gain a significant competitive edge.
These practices will have long-term scalability, seamless data access, and adaptable interoperable ecosystems ready for future growth. So, the faster you align your systems to the EHR integration requirements under the 21st Century Cures Act, the better your advantage will be.
So, what are you waiting for? Talk to our experts, get your interoperability maturity assessment, and start transforming your healthcare ecosystem.
Frequently Asked Questions
The 21st Century Cures Act requires EHRs to support standardized API access, prevent information blocking, and enable full Electronic Health Information (EHI) exchange. By 2026, systems must align with USCDI standards, provide patient-accessible data, and meet updated ONC certification and HTI-1 compliance requirements.
Legacy interface engines built on HL7 often lack support for modern API-based interoperability. Compliance requires adding FHIR layers, upgrading data models, or introducing middleware. Many systems must shift from point-to-point integrations to platform-based architectures, increasing complexity, cost, and modernization effort.
Standardized APIs, particularly FHIR, ensure consistent, secure, and real-time access to health data. By eliminating custom access barriers and enabling third-party connectivity, APIs reduce the risk of information blocking and ensure compliance with mandated data access and exchange requirements.
The ONC certification now emphasizes real-world interoperability, standardized API functionality, and EHI access. Recent updates include stricter testing, transparency requirements for decision support tools, and alignment with USCDI and HTI-1 rules to ensure systems meet evolving compliance expectations.
Failure to comply with patient data access rules may be classified as information blocking. Penalties can include financial disincentives, loss of certification, exclusion from federal programs, and reputational risk. Enforcement varies by actor type, but compliance is increasingly tied to operational and financial viability.
The 21st Century Cures Act requires EHRs to allow patients to access their data via third-party apps of their choice. This mandates secure API-based connectivity, supports app ecosystems, and shifts control of data access toward patients while maintaining provider responsibility for secure data exchange.
Federal interoperability rules under the Cures Act generally do not override stricter state privacy laws. Instead, organizations must comply with both. If state laws impose tighter restrictions, they take precedence, requiring careful alignment between federal data-sharing mandates and local privacy regulations.
There is no single mandated audit deadline, but organizations are expected to maintain continuous compliance. Most health systems conduct internal audits annually or during major upgrades. With HTI-1 milestones approaching in 2026, proactive assessments in 2025–2026 are critical to avoid compliance gaps.
- On April 2, 2026
- 0 Comment

