
How to Build an AI-Powered EHR
Did you know that by 2024, nearly 71% of hospitals had integrated predictive AI in their EHRs?
This adoption shows that today, EHRs have long grown from just documentation software to more intelligent systems that think, predict, and guide. However, when it comes to supporting these AI capabilities, many traditional EHRs fall short.
The reason is that traditional EHRs are built on a rigid architecture, static workflows, and fragmented data models. Yet, many EHRs try to retrofit onto legacy architectures, resulting in fragmented workflows, unreliable predictions, and clinician burnout.
At the same time, generative AI in healthcare software is reshaping how EHRs are built, not just how they are used. Moreover, large language models, predictive analytics, and real-time interfaces are pushing healthcare organizations to rethink platform architecture, interoperability, and governance from the ground up.
This is why many forward-looking organizations are exploring AI EHR development strategies that go beyond vendor roadmaps and focus on building intelligent, future-ready systems. In some cases, this even means choosing to build your own EHR to retain control over data, workflows, and AI models.
In this guide, we will walk you through how to build an AI-powered EHR with a practical, system-level perspective. It covers strategic planning, healthcare AI platform architecture, FHIR-based data pipelines for healthcare AI, AI-native clinical workflows, LLM integration patterns, and security-by-design considerations.
Let’s help you move from documentation-first systems to truly intelligent EHR platforms.
Planning Your AI-Powered EHR Strategy
Building an AI-powered EHR starts long before models, algorithms, or integrations. Without a clear strategy, AI features quickly turn into isolated experiments that fail to deliver clinical or operational value.
The planning phase is where you define who the system is for, what intelligence it should deliver, and how much control your organization needs over data and AI behavior. Here is how you can plan the whole AI EHR development process:
- Define Core User Personas Early: An AI-powered EHR must serve multiple personas with very different needs. Clinicians prioritize speed, clinical relevance, and minimal disruption, while operational teams focus on efficiency, compliance, and reporting. Defining these personas early ensures AI supports real workflows rather than introducing friction or cognitive overload.
- Identify AI-First Use Cases at a System Level: Instead of starting with individual AI features, focus on system-level intelligence. For instance, predictive risk scoring across patient populations, automated clinical summarization, workflow prioritization, and proactive care gap identification. These use cases shape architectural and data decisions far more effectively than feature checklists.
- Decide Whether to Build or Extend Your EHR: For organizations with complex workflows or long-term AI ambitions, many are choosing to build their own EHR rather than relying solely on vendor platforms. This approach offers greater control over data pipelines, model governance, and AI customization, critical factors for scaling intelligence safely and sustainably.
- Align AI Strategy With Clinical & Regulatory Realities: AI behavior must reflect real-world clinical workflows, regulatory requirements, and risk tolerance. That’s why the planning should include governance models, human-in-the-loop validation, and compliance considerations from day one.
In short, a strong strategy sets the foundation for everything that follows; without it, even the most advanced AI cannot deliver meaningful impact inside an EHR.
Healthcare AI Platform Architecture: The Foundation
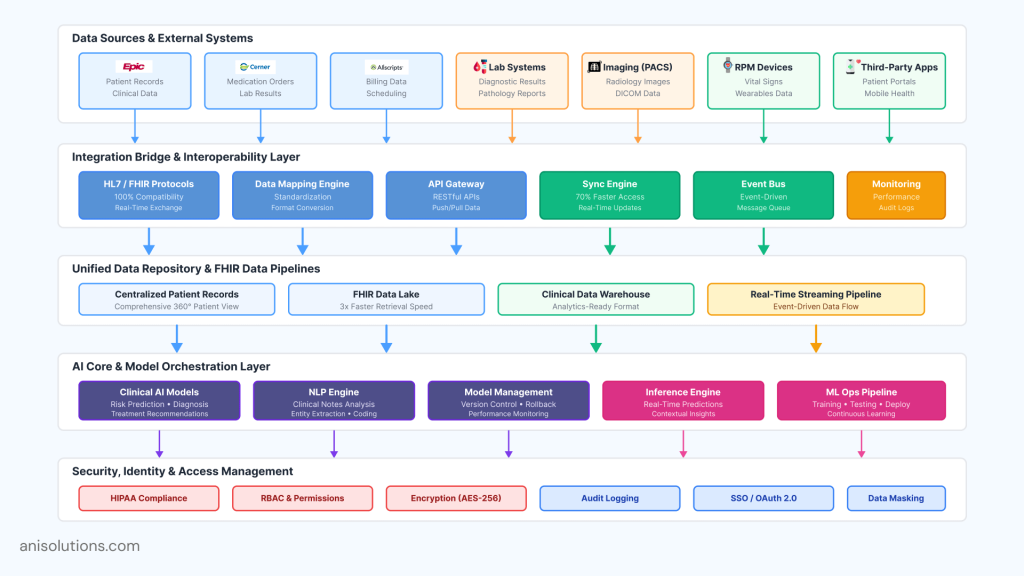
An AI-powered EHR cannot be built on top of a traditional, monolithic architecture, and does not allow an platform level integration. Without an AI-ready foundation, even well-trained models fail to deliver reliable insights, real-time responses, or clinical trust. Architecture is what determines whether AI remains or becomes operational at scale.
- Embed AI at the Architecture Layer: The AI needs to be a core ability, not just an add-on for the EHR. This means designing systems where data flows, workflows, and permissions are optimized for continuous analysis, feedback, and learning, rather than batch processing or isolated analytics.
- Design for Data Ingestion & Interoperability: AI tools depend on timely, high-quality data to work on their full potential. That’s why AI-ready EHR must support seamless ingestion from internal modules and external sources such as labs, imaging systems, RPM devices, and third-party applications.
- Enable Model Orchestration & Lifecycle Management: Over time, as AI usage grows, multiple models will coexist across clinical and operational workflows. The platform must support model versioning, monitoring, rollback, and performance tracking to ensure safety, reliability, and continuous improvement.
- Build Secure Access & Identity Management: AI inference must respect clinical roles, permissions, and data sensitivity. Strong identity management, role-based access control, and auditability ensure that AI outputs are delivered securely and appropriately across users and workflows.
- Use FHIR-Based Data Pipelines for Real-Time Intelligence: FHIR-based data pipelines for healthcare AI enable standardized, event-driven data exchange, enabling real-time predictions and contextual insights within clinical workflows.
Want to Build AI-Ready Architecture? Get Your Checklist
Assess NowDeveloping AI-Native Clinical Workflows
Most EHR platforms today stop at AI-assisted workflows, which add recommendations, alerts, or summaries on top of the existing process. While helpful, this approach often increases cognitive load and workflow fragmentation.
On the other hand, AI-native clinical workflows completely redesign how work happens, so intelligence operates continuously in the background. This way, the system supports clinicians without demanding constant interaction.
The difference between AI-assisted and AI-native workflows becomes clearer when viewed at the workflow level rather than the feature level.
| Dimension | AI-Assisted Workflows | AI-Native Clinical Workflows |
| Workflow design | AI supports existing manual steps | Workflows are redesigned around intelligence |
| Data capture | Manual entry triggers AI analysis | Continuous, background data ingestion |
| Clinician interaction | Frequent prompts and alerts | Minimal interruptions, context-aware insights |
| Decision support | Reactive recommendations | Proactive, predictive guidance |
| Cognitive load | Often increases with more alerts | Reduced through automation and prioritization |
| Clinical trust | Limited by explainability gaps | Built through transparency and validation |
| Scalability | Difficult to extend across workflows | Designed to scale across care pathways |
When building intelligent EHR systems, AI-native workflows transform AI from a disruptive tool into a quiet partner, enhancing care delivery without changing how medicine is practiced.
Security, Privacy, & Compliance by Design
The AI-native clinical workflows need to be built through security, privacy, and compliance embedded directly into the design. In an AI-powered EHR, this also helps in increasing the transparency and trust of the clinicians.
- Embed Security Into AI Workflows: Security must extend beyond data storage to how AI operates within workflows. This includes controlling which models can access specific data, enforcing least-privilege access during inference, and securing every AI-driven interaction across the platform. Without this, intelligence quickly becomes a source of risk.
- Apply Role-Based Access & End-to-End Auditability: AI-generated insights should follow the same access controls as clinical data. Role-based permissions ensure that only authorized users can view or act on AI outputs. Additionally, every action from data access and model execution to recommendation delivery must be logged to support accountability, monitoring, and regulatory review.
- Protect PHI Throughout AI Inference: AI inference introduces new exposure points for protected health information. Sensitive data must remain encrypted in transit, at rest, and during processing. Clear separation between clinical data, model inputs, and outputs helps reduce leakage and limits unintended reuse.
- Design for Compliance From the Start: Regulatory readiness cannot be retrofitted and needs to be integrated from the start. AI-powered EHRs must support explainability, traceability, and documentation that aligns with HIPAA and interoperability requirements. Governance frameworks should define how models are validated, updated, and monitored over time.
By embedding security and compliance into the EHR platform itself, organizations create a trusted foundation for AI at scale. This enables advanced capabilities without compromising safety, clinical integrity, or regulatory confidence.
Integrating LLMs into the EHR Platform
One of the best tools that adds significant value to healthcare is LLMs or large language models, but only when they are integrated safely and seamlessly. In an AI-powered EHR, LLMs should enhance clinical workflows without becoming decision-makers themselves. Their role is to reduce cognitive burden, surface context, and support clinicians, not to replace clinical judgement.
Let’s take a look at how to integrate LLMs into electronic health records:
- Use LLMs Where Language, Not Prediction, Is the Problem: LLMs are best suited for tasks involving language and context, such as clinical note summarization, chart review assistance, and contextual data retrieval. They should not be used for deterministic clinical decisions or risk scoring, which are better suited for predictive models.
- Integrate LLMs Using Safe Architectural Patterns: The LLMs should operate behind secure service layers rather than accessing raw EHR databases directly. It can be done through controlled APIs, scoped permissions, and intermediary services that help ensure that LLM interactions remain auditable, explainable, and compliant with healthcare regulations.
- Rely on Retrivel-Augmented Generation (RAG): Using RAG allows LLMs to generate responses grounded in verified clinical data rather than relying on model memory alone. By retrieving relevant patient context, guidelines, or historical records at runtime, RAG improves accuracy while reducing hallucination risk.
- Maintain Clinical Trust & Oversight: LLM outputs must be clearly distinguishable from clinician-authored content. Systems should provide visibility into source data, allow easy validation or correction, and ensure that final clinical decisions always remain with human providers.
Download the LLM Integration Requirement Checklist to Automate Patient Engagement
Get NowKey Challenges in AI-Powered EHR Development
Building an AI-powered EHR introduces challenges that go beyond model performance. Many failures occur not because AI is ineffective, but because foundational issues are overlooked during design and implementation. Addressing these challenges early is essential for delivering safe, scalable, and clinically useful intelligence.
- Solving Data Quality & Silo Issues: AI systems are only as reliable as the data they consume. Inconsistent data formats, incomplete records, and siloed systems undermine model accuracy and trust. Before deploying AI, organizations must standardize data, resolve interoperability gaps, and ensure reliable data pipelines across clinical and operational systems.
- Managing Bias, Transparency, & Explainability: AI models can unintentionally reinforce bias if training data is unbalanced or poorly representative. Without transparency, clinicians may struggle to understand or trust AI recommendations. AI-powered EHRs must support explainable outputs, clear reasoning paths, and ongoing monitoring to detect and correct bias over time.
- Aligning AI With Real-World Clinical Workflows: Even accurate AI fails if it disrupts clinical practice. Models must operate within real clinical constraints, accounting for time pressure, incomplete information, and varying care pathways. In this, close collaboration with clinicians during design and testing ensures AI outputs are relevant, timely, and actionable.
Conclusion: Building an EHR That Is Ready for AI at Scale
Long story short, AI-powered EHRs are built on architecture and not only the features. To build these systems, you need to plan everything from strategy to architecture to workflows, security, and governance, and every layer determines whether AI delivers real clinical value.
When intelligence is embedded thoughtfully, AI becomes a trusted partner that enhances care delivery without compromising safety or clinical judgment. As healthcare continues to shift toward intelligence-driven systems, organizations that invest in AI-ready EHR foundations today will be positioned to scale innovation responsibly and sustainably.
Ready to build an AI-powered EHR tailored to your needs? Click here to get started.
Frequently Asked Questions
Q. How do you build an AI-powered EHR from scratch?
Building an AI-powered EHR starts with AI-first planning, interoperable data pipelines, and modular architecture. Intelligence must be embedded into workflows, security, and governance layers rather than added as isolated features.
Q. What architecture is required to support AI in EHR development?
AI-powered EHRs require modular, cloud-ready architecture with real-time data ingestion, FHIR-based interoperability, model orchestration layers, and strong identity and access management to support scalable, secure intelligence.
Q. How can LLMs be safely integrated into electronic health records?
LLMs should be integrated through controlled service layers using retrieval-augmented generation (RAG), scoped access, and auditability. They must support clinicians with language tasks while preserving human oversight and clinical accountability.
Q. What are AI-native clinical workflows and why do they matter?
AI-native clinical workflows are designed around continuous intelligence rather than manual steps. They reduce cognitive load, minimize documentation burden, and deliver proactive insights while keeping clinicians in control of final decisions.
Q. How do you ensure security and compliance in AI-powered EHR systems?
Security and compliance must be built into AI workflows using role-based access, encryption, audit trails, and model traceability. Designing for HIPAA and interoperability from the start ensures safe, scalable AI deployment.
Building an AI-powered EHR starts with AI-first planning, interoperable data pipelines, and modular architecture. Intelligence must be embedded into workflows, security, and governance layers rather than added as isolated features.
AI-powered EHRs require modular, cloud-ready architecture with real-time data ingestion, FHIR-based interoperability, model orchestration layers, and strong identity and access management to support scalable, secure intelligence.
LLMs should be integrated through controlled service layers using retrieval-augmented generation (RAG), scoped access, and auditability. They must support clinicians with language tasks while preserving human oversight and clinical accountability.
AI-native clinical workflows are designed around continuous intelligence rather than manual steps. They reduce cognitive load, minimize documentation burden, and deliver proactive insights while keeping clinicians in control of final decisions.
Security and compliance must be built into AI workflows using role-based access, encryption, audit trails, and model traceability. Designing for HIPAA and interoperability from the start ensures safe, scalable AI deployment.
- On February 13, 2026
- 0 Comment

