
FHIR R4 vs HL7 v2: When to Use Each Standard for Healthcare Data Exchange
One builds the foundation for data exchange internally, and the other evolves this data exchange to true interoperability. Yet, many assume that HL7 v2 is slowly being replaced by FHIR API standards.
Although if you look at nearly 90% of hospitals using APIs for data exchange, it looks like that. But we also need to look at the other side of the coin, because despite this shift, HL7 v2 is still powering core workflows such as admission, lab reporting, and order management.
Most importantly, this shift is about how the data is exchanged. The HL7 v2 functions on a push model, which sends data after any event happens. Whereas, FHIR standard functions on a pull model, allowing systems to request patient data when needed. This transformation enables a more flexible, scalable, and developer-friendly healthcare ecosystem.
So, one thing you must remember is that FHIR is not a replacement for HL7 v2; it’s a way to evolve HL7 v2 beyond its limits.
Moreover, they both have their own strong points, and according to them, where they are used changes. And this is something that you must understand before designing your EHR if you are a healthcare CTO or developer.
That’s why, in this blog, we will understand how these two standards work, compare their differences, and help you decide when to use HL7 v2 vs FHIR to build a scalable and interoperable system.
How They Work: FHIR API Standard vs HL7 v2 Messaging Standard
The best way to understand the difference between HL7 v2 and FHIR is to know how they work. These two standards were developed by HL7 International; they function on different data exchange models. Let’s take a look at those models:
- How HL7 v2 Works?
HL7 v2 is a messaging standard that works on a push model, meaning when an event is triggered, a message is generated and sent to one healthcare system from another healthcare system. For example, a new patient is admitted, and a message is sent from the receptionist desk to the EHR to create a patient profile.
Additionally, these messages are in a pipe-delimited format. This format is efficient for system-to-system communication, but it can be difficult to interpret and customize. However, the HL7 v2 is highly reliable despite its complexity and is used as the core for hospital systems.
This is an example of how the pipe-delimited format looks:
- MSH|^~\&|…
- PID|12345|…
- How FHIR Standards Work?
The FHIR R4 standard works on RESTful APIs for exchanging data between systems. With this API-driven architecture, it shifts to a pull model, meaning instead of event-driven exchange, systems can request specific healthcare data from other systems.
The information is structured into different resources such as Patient, Observation, and Medication. This makes it easier to share the data in real-time and without sharing entire patient profiles, making the data exchange faster.
Key Differences: FHIR R4 vs HL7 v2
After understanding how these two standards function, let’s understand some other factors, such as data formats, interoperability, and system design, that differentiate FHIR R4 and HL7 v2, other than just their architecture:
| Aspect | FHIR R4 | HL7 v2 |
| Data Format | JSON/XML (structured resources) | Pipe-delimited messages |
| Communication Model | RESTful APIs (pull-based) | Event-driven messaging (push-based) |
| Interoperability | High standardization | Implementation-specific |
| Developer Experience | Modern, API-friendly | Complex, legacy-heavy |
| Scalability | High (web-scale ecosystems) | Limited for modern use cases |
- Data Format
This is the first differentiator, as HL7 v2 uses pipe-delimited format for messaging. These are compact and efficient but often difficult to understand and interpret as the structure can vary across implementations, making standardization challenging.
Whereas FHIR is based on JSPN and XML, and organizes data into defined resources, making it more readable, consistent, and developer-friendly.
- Communication Model
After the data model, the next difference is that HL7 v2 functions on an event-driven model, where data is sent after an event, such as patient admission or lab order, is triggered.
On the other hand, FHIR uses APIs enabling real-time data exchange between systems by allowing systems to send requests to get data when needed, giving more flexibility and control.
- Interoperability
With HL7 v2, interoperability requires each new custom integration due to differences in implementation, which can limit seamless data exchange.
However, FHIR interoperability with standardized APIs and data models enables more consistent communication across multiple systems.
- Developer Experience
When it comes to developing HL7 v2, it involves handling complex message formats and interface engines, making development and maintenance more challenging.
Whereas FHIR is powered by modern API standards, reducing complexity and accelerating application development, it simplifies the development process for developers.
- Scalability & Flexibility
HL7 v2 is highly effective for internal, high-volume workflows but is less suited for modern, API-driven use cases.
However, the FHIR API standard is designed for scalability, supporting applications, analytics, and real-time data access across connected systems.
In short, the difference between HL7 v2 and FHIR R4 is not about capability but how healthcare systems exchange and use data.
Pros & Cons of FHIR R4 & HL7 v2
Before understanding when to use HL7 v2 and FHIR in healthcare, it is important to clarify the pros and cons of each standard. Because if you don’t understand strengths and weaknesses, then defining use cases will not be easy, and one wrong choice can break the interoperability in the healthcare ecosystem:
So, let’s look at the pros and cons of FHIR R4 for healthcare data exchange along with HL7 v2:
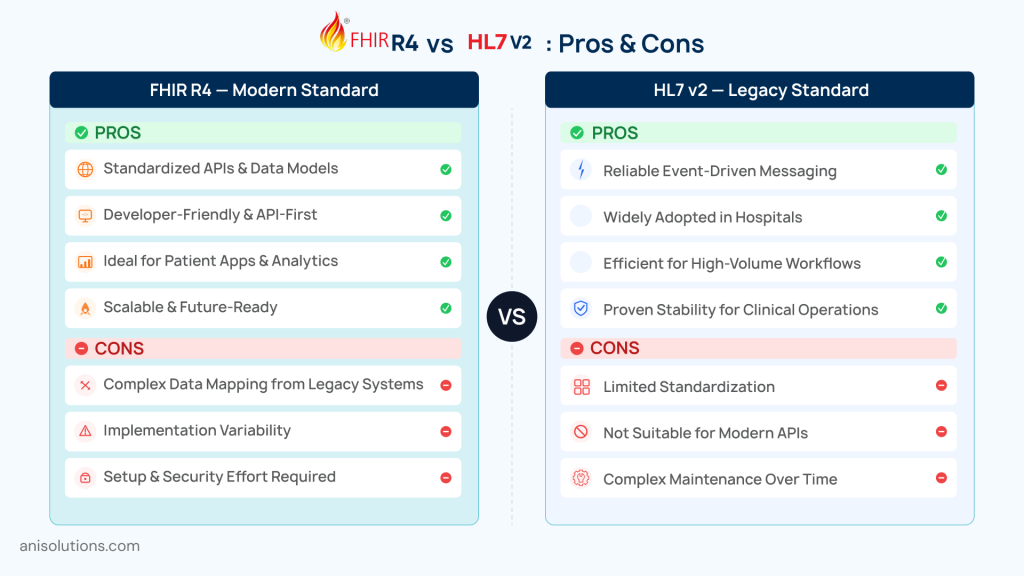
FHIR R4- Pros:
- Enables strong FHIR interoperability through standardized APIs and data models.
- API-first and developer-friendly, simplifying modern healthcare app development.
- Ideal for patient-facing applications, analytics, and real-time data access.
- Supports scalable, flexible, and future-ready healthcare ecosystems.
FHIR R4- Cons
- Data mapping from legacy systems such as HL7 v2 can be complex and resource-intensive.
- Implementation variability across vendors can affect consistency.
- Requires initial setup effort, including infrastructure and security configuration.
HL7 v2- Pros
- Highly reliable for real-time, event-driven messaging across systems.
- Deeply embedded in hospital infrastructure and widely adopted.
- Efficient for high-volume workflows such as admissions, lab results, and orders.
- Proven stability for urgent clinical operations.
HL7 v2- Cons
- Limited standardization across implementation, leading to customization challenges.
- Not well-suited for modern API-driven use cases or external integrations.
- Maintenance and interface management can become complex over time.
In short, FHIR R4 is best for enabling innovation and interoperability, while HL7 v2 is essential for supporting core operations. So, the choice between them depends on whether the goal is to modernize systems or maintain efficient internal data exchange.
Challenges in Adopting FHIR vs HL7 v2
While it is necessary to either adopt FHIR R4 entirely or alongside the HL7 v2, it is not a simple process. Healthcare organizations face several challenges while transitioning the systems, including data, systems, and cost considerations. Here are some of the challenges:
- Data Mapping Complexity
One of the biggest challenges is to map HL7 v2 messages to FHIR resources. These two standards function on completely different models, and there is no one-to-one mapping; this leads to inconsistencies in data structure and missing data fields. Because of this, the process becomes complex and the most time-consuming part of the transformation.
- Vendor-Specific Implementation
Another challenge is the different EHRs in how they implement APIs, structure data, and scope the data. This means that with each system, the approach to the transformation process changes, requiring additional customization and testing, making it difficult to complete the process early.
- Migration Cost vs Maintenance Trade-Off
Migrating data from one system to another is quite a costly process, and balancing it with ongoing maintenance costs is difficult. While HL7 v2 has a lower maintenance cost, the custom interfaces for each connection are expensive compared to an API-based FHIR architecture.
- Performance Trade-Offs
Finally, the HL7 v2 is best for high-volume, event-driven messaging, making it efficient for internal workflows. Whereas FHIR’s API-based approach may have some latency issues for high-volume data exchange because of its request-based model, especially in large-scale environments.
Decision Matrix: When to Use HL7 v2 vs FHIR in Healthcare
By now, you might have understood where you need to use it; however, let’s take a look at use cases based on system requirements and long-term interoperability goals. So, rather than only choosing based on their models or comparing old vs new standards, it’s important to choose based on what you need and what suits your clinic:
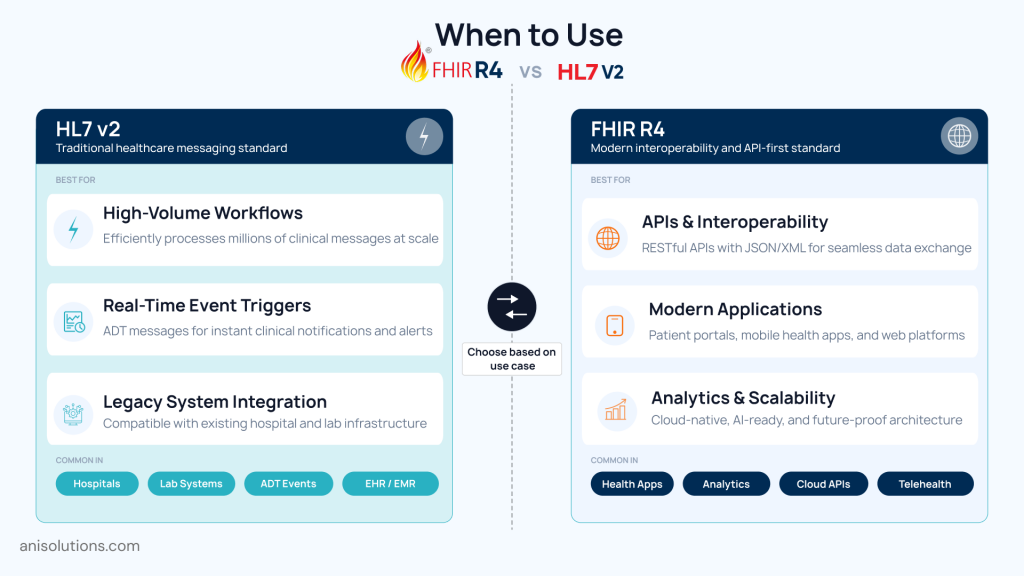
Use HL7 v2 When:
- Managing high-volume internal workflows such as admission, discharge, transfer, or lab results.
- Real-time, event-driven data exchange is important for operations.
- Working within legacy infrastructure that is deeply embedded in hospital systems.
Using HL7 remains most reliable if you need to handle system core operational workflows or transfer large-scale data while maintaining consistency and speed.
Use FHIR R4 When:
- Building modern applications, including patient-facing and provider-facing tools.
- Enabling interoperability across multiple systems using standardized APIs.
- Supporting analytics, population health management, and API-driven ecosystems.
So, FHIR is the best choice to improve system interoperability and use cases that require flexibility, scalability, and real-time data access across the ecosystem.
Hybrid Approach:
This is the most effective approach in real-world practices as it maintains continuity of operations while bringing capabilities of the FHIR standard through APIs. In this approach, you can wrap FHIR APIs on the HL7 v2, leading to HL7 v2 handling internal workflows while the FHIR standard expands the interoperability.
Strategic Outlook: The Future of Healthcare Data Exchange
As mentioned in the introduction, the healthcare data exchange is shifting from message-driven systems to API-driven ecosystems. And at the center of this is the FHIR API standard, which is becoming standardized rapidly.
Moreover, regulations such as the 21st Century Cures Act are also pushing for open data access and adoption of FHIR. However, this emerging FHIR standard does not replace the HL7 v2, as this standard is essential for core operations of the healthcare ecosystem.
HL7 v2 is reliable and able to exchange large-scale data across systems much faster than FHIR’s resource-based model. The best choice is to combine the capabilities of both FHIR R4 and HL7 v2.
With this hybrid approach, you get a reliable core system powered by HL7 v2 and interoperability, flexibility, and scalability of FHIR APIs without disrupting existing operations.
In short, healthcare interoperability does not mean replacing old standards with new ones; it means balancing every standard to build a connected, flexible, and scalable ecosystem.
Conclusion: Choosing the Right Integration Backbone
Although FHIR R4 is an emerging standard and almost all healthcare organizations are adopting APIs to exchange health data, HL7 v2 is not replaceable. It is crucial for internal workflows functioning, and it is the operational backbone of the healthcare ecosystem.
So, the best course of action for healthcare organizations is to take a hybrid approach where HL7 v2 and FHIR R4 work alongside each other. With this, the systems can flexibly share data while continuing their existing operations without disruption from transitioning.
At A&I Solutions, our developers are experts at building EHR integrations that combine the abilities of both standards. If you want to take a more practical approach to your EHR integrations, then Talk to our EHR integration experts to assess your system and start your modernization journey today.
Frequently Asked Questions
The difference between FHIR R4 and HL7 v2 lies in how they exchange data. HL7 v2 uses event-driven, push-based messaging, while FHIR uses API-driven, pull-based access with structured resources, enabling more flexible, scalable, and developer-friendly interoperability.
Healthcare organizations should use HL7 v2 for high-volume internal workflows like admissions, lab results, and order messaging. It is ideal when real-time event-driven communication is critical and when working within legacy systems that are deeply embedded in hospital operations.
FHIR is better suited for modern applications because it uses standardized APIs, supports real-time data access, and offers structured, developer-friendly formats like JSON. This enables faster development, seamless integration, and scalable solutions for patient apps, analytics, and interoperable healthcare ecosystems.
HL7 v2 typically relies on network-level security and trusted environments, with limited built-in authentication mechanisms. In contrast, FHIR APIs use modern security protocols like OAuth 2.0 and role-based access, enabling secure, granular, and standardized control over patient data access.
Yes, HL7 v2 and FHIR commonly coexist in hybrid architectures. HL7 v2 handles internal workflows, while FHIR APIs expose data for external applications, enabling interoperability without replacing existing systems.
FHIR R4 is currently the most widely adopted and stable version for enterprise use. It is supported by major EHR vendors, aligns with regulatory requirements, and provides a consistent foundation for building interoperable healthcare applications.
SMART on FHIR apps cannot directly interact with HL7 v2 systems. However, organizations can use FHIR APIs as a layer on top of HL7 v2 infrastructure, enabling SMART apps to access and use data indirectly through standardized interfaces.
Maintaining HL7 v2 often involves ongoing costs due to custom interfaces and integration complexity. While adopting FHIR requires higher upfront investment, it reduces long-term costs through standardized APIs, easier scalability, and lower maintenance overhead for modern, interoperable healthcare systems.
- On April 14, 2026
- 0 Comment

