
Legacy HL7 v2 to FHIR R4 Migration: Technical Roadmap & Common Pitfalls
For decades, organizations transferred data from one system to another by using the HL7 v2 messaging standard. In fact, according to HL7 International, nearly 95% of healthcare organizations are still using HL7 v2 to transfer data.
And honestly, the reason for this is pretty clear, as hospitals have relied on HL7 v2 for ADT workflows, lab orders, and countless other clinical operations. However, today’s healthcare interoperability is completely different, and HL7 v2 was not designed for this.
What the modern healthcare organization needs is real-time APIs, cloud interoperability, patient-facing apps, payer connectivity, and scalable data exchange. This is where FHIR APIs fulfill all these needs, and this is the reason why 78% of healthcare organizations have implemented FHIR APIs.
But this is where the real challenge begins in HL7 v2 to FHIR R4 migration. Because you can’t replace HL7 overnight, as they are the core of interoperability operations. You have to make them work together; this is not as easy as it may look.
That’s why the best approach is to keep HL7 v2 for managing internal workflows and expand FHIR R4 APIs for supporting and expanding modern interoperability. However, achieving this balance is far more complicated than basic data transformation.
And for this, you need a robust HL7 v2 to FHIR R4 migration roadmap to build an interoperability architecture, terminology mapping, governance, transformation workflows, and API orchestration without disrupting ongoing healthcare operations.
So, in this guide, we will walk you through the approach to legacy HL7 data transformation, how to map legacy HL7 segments to FHIR resources, and technical pitfalls in HL7 to FHIR data transformation to help you build a migration strategy that supports long-term API-driven healthcare interoperability.
Planning an HL7 to FHIR Migration Roadmap
After you decide to modernize your healthcare interoperability, the next step is to figure out the actual HL7 v2 to FHIR R4 migration roadmap for healthcare systems. And for this, the first thing you need to understand is that FHIR modernization is not just about enabling APIs.
This requires careful planning for interoperability continuity, transformation workflows, governance, and long-term scalability. So, for this, the first decision you need to make is which migration model is right for you. You may choose:
- Real-time transformation models.
- Batch migration workflows.
- Hybrid interoperability approaches.
In these models, real-time transformations are used if you want live interoperability, and for this, continuous HL7-to-FHIR conversion during active clinical operations. Whereas batch migration is best for transferring historical and archived data, as immediate synchronization is not necessary.
However, the best approach that many of our clients and other healthcare organizations choose hybrid migration model. This model combines both approaches that reduce operational risks, and it also supports phased modernization.
Another point is infrastructure readiness and FHIR converter implementation planning. You must evaluate whether the interface engines, APIs, middleware, and interoperability platforms can support large-scale transformation workflows without creating latency or synchronization issues.
Planning for governance and monitoring is also crucial for successful HL7 v2 to FHIR migration. In this stage, you have to define rollback strategy, interoperability monitoring strategies, validation processes, security controls, and operational ownership before the migration process even begins.
Because the HL7 v2 is not replaceable in just a few months, and it needs to work seamlessly with FHIR R4 for years as the interoperability standard evolves. This is why an effective HL7 v2 to FHIR R4 migration roadmap is phased rather than disruptive.
So, the best course of action is to keep both interoperability workflows working simultaneously. You must prioritize high-impact APIs, patient-facing applications, cloud integrations, and external interoperability services first and then gradually modernize your legacy HL7 workflows over time.
Mapping & Normalization Legacy HL7 Data
One of the most challenging yet important parts of the migration process is mapping HL7 v2 to FHIR resources. Without careful mapping, maintaining the interoperability context and clinical meaning becomes quite difficult.
And this is why FHIR modernization is more than just field-to-field transformation. More importantly, the HL7 v2 workflows are event-driven, whereas FHIR R4 is modular and API-based. This architectural difference means you need to redesign how healthcare data is structured, accessed, validated, and exchanged during transformation.
Some of the most common HL7 v2 to FHIR mappings include:
| HL7 v2 Segment | FHIR R4 Resource | Migration Purpose |
| PID | Patient | Patient demographics and identifiers |
| PV1 | Encounter | Visit and encounter details |
| OBX | Observation | Clinical observations and lab results |
| ORC/RXE | MedicationRequest | Medication orders and prescriptions |
| AL1 | AllergyIntolerance | Allergy and sensitivity records |
| DG1 | Condition | Diagnosis and problem list mapping |
However, these mappings are rarely easy or straightforward to complete. Because a single HL7 message may connect multiple FHIR resources, while multiple workflows may need to be consolidated into a single interoperability process.
Additionally, transforming custom Z-segments and composite data types is another challenge. Many healthcare organizations have created their own localized HL7 extensions over the years to support custom workflows, operational requirements, or vendor-specific logic. These data types require new transformation rules and FHIR extensions during modernization.
Normalization is another critical factor during migration, as legacy code systems frequently need to be translated into standardized vocabularies like LOINC, SNOMED CT, and RxNorm to support scalable interoperability and API consistency.
Many healthcare organizations are now also using AI-assisted mapping tools to accelerate transformation workflows, identify semantic mismatches, and improve interoperability validation during large-scale healthcare modernization initiatives.
Common Technical Pitfalls in HL7 to FHIR Migration
Even with a structured HL7 v2 to FHIR R4 migration strategy, healthcare organizations often encounter technical challenges that can slow modernization efforts or disrupt interoperability workflows.
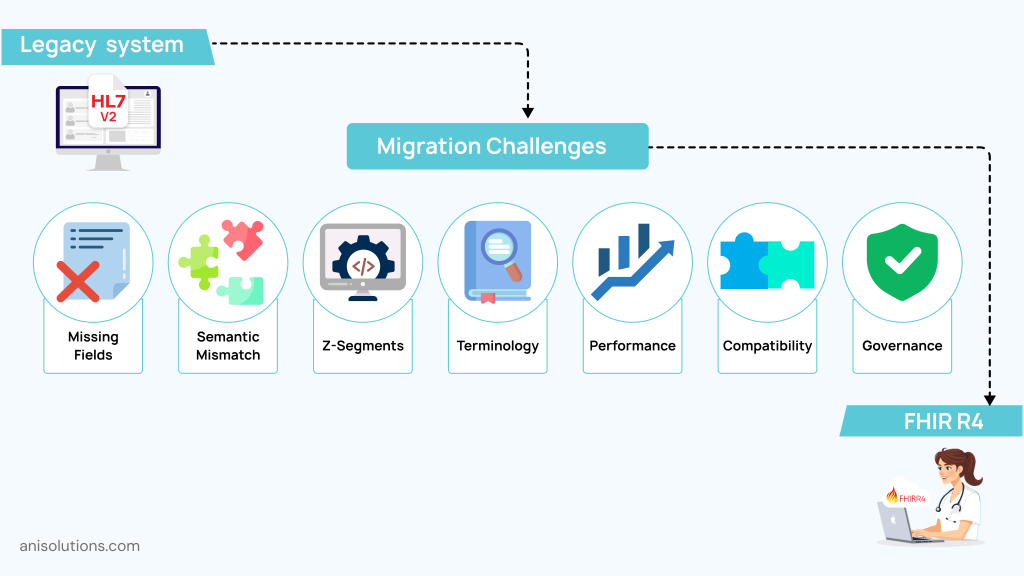
And, most of these challenges happen because HL7 v2 and FHIR R4 follow very different interoperability models. Some of the most common technical pitfalls include:
- Missing Required FHIR Fields: Legacy HL7 messages may not always contain the identifiers, references, or structured relationships required for valid FHIR resources, leading to failed validations and incomplete API responses.
- Semantic Mismatches Between HL7 & FHIR: HL7 workflows are event-driven, while FHIR is resource-based. This creates interoperability challenges when organizations try to preserve workflow meaning during transformation.
- Custom Z-Segment Complexity: Many hospitals use custom Z-segments for localized workflows and vendor-specific logic. These often require custom FHIR extensions and specialized transformation rules during migration.
- Terminology Normalization Issues: Legacy code systems frequently need mapping into standardized vocabularies like LOINC, SNOMED CT, and RxNorm to support scalable interoperability.
- Performance Bottlenecks in Real-Time Pipelines: Continuous HL7-to-FHIR transformation can create API latency, synchronization delays, and throughput limitations in high-volume healthcare environments.
- Backward Compatibility Challenges: Most organizations must maintain legacy HL7 workflows while gradually introducing FHIR APIs, creating hybrid interoperability environments that are operationally difficult to manage.
- Governance & Validation Gaps: Without strong interoperability governance, organizations may struggle with inconsistent mappings, API reliability issues, and incomplete transformation validation during production rollout.
This is why phased testing, interoperability monitoring, and continuous validation become critical throughout healthcare modernization initiatives.
Validation & Production Readiness
Once transformation workflows are implemented, healthcare organizations need to validate whether the new interoperability environment can actually support production-scale operations reliably. Because honestly, successful hl7 v2 to fhir r4 migration is not just about converting data correctly. It is about ensuring interoperability remains stable, accurate, secure, and scalable under real healthcare workloads.
One of the first priorities during this stage is interoperability and schema validation. Organizations need to test whether transformed FHIR resources follow proper formatting, maintain required references, and preserve clinical meaning across APIs, workflows, and connected healthcare systems.
Some of the most important validation areas include:
- FHIR Schema Validation
Ensuring transformed resources meet FHIR R4 structural and formatting requirements without missing mandatory fields or invalid references. - US Core Profile Conformance
Validating interoperability workflows against US Core implementation standards to support broader healthcare interoperability readiness. - API Reliability Testing
Monitoring response times, throughput, authentication workflows, and scalability under real-time healthcare interoperability conditions. - Synchronization Accuracy Monitoring
Confirming that transformed data remains consistent across HL7 and FHIR environments during phased modernization and coexistence periods. - Regression and Transformation Testing
Using automated message simulators and interoperability testing tools to validate transformation logic across multiple clinical workflows and edge-case scenarios. - Security and Access Validation
Verifying API security controls, audit logging, authentication policies, and protected health information safeguards throughout production rollout.
Many healthcare organizations also use automated interoperability monitoring tools to detect transformation anomalies, schema inconsistencies, synchronization delays, and API failures before they affect production environments.
Because honestly, production readiness is not only about making FHIR APIs functional. It is about ensuring the entire interoperability pipeline remains reliable enough to support real-world healthcare operations continuously and securely.
Conclusion: Building a Future-Ready Interoperability Pipeline
In a nutshell, an effective HL7 v2 to FHIR R4 migration is not simply about replacing one interoperability standard with another. It is about modernizing healthcare integration architecture in a way that supports scalability, API-driven interoperability, operational continuity, and long-term digital transformation goals.
And honestly, successful modernization rarely happens through direct replacement alone. Most healthcare organizations need phased migration strategies, strong governance, terminology normalization, interoperability validation, and hybrid HL7-FHIR coexistence environments to modernize safely without disrupting existing workflows.
As healthcare ecosystems continue evolving toward real-time APIs, cloud interoperability, and AI-driven healthcare operations, organizations that modernize their interoperability infrastructure today will be far better prepared for future innovation and interoperability demands.
At A&I Solutions, our healthcare modernization and integration capabilities help organizations build scalable interoperability ecosystems through secure HL7 modernization, FHIR integration, interface transformation, and future-ready healthcare connectivity strategies.
Frequently Asked Questions
HL7 v2 uses event-driven messaging for system-to-system communication, while FHIR R4 uses modular API-based resources designed for real-time interoperability, cloud integration, and modern healthcare application connectivity.
Healthcare organizations are adopting FHIR R4 to support API-first interoperability, patient-facing applications, cloud scalability, payer connectivity, and real-time healthcare data exchange while modernizing beyond traditional HL7 message-based interoperability workflows.
An HL7 to FHIR migration roadmap should include interoperability assessment, infrastructure planning, transformation workflows, terminology normalization, governance policies, rollback planning, validation strategies, API readiness, and phased modernization approaches that maintain operational continuity during migration.
Healthcare organizations map legacy HL7 segments by transforming message-based workflows into structured FHIR resources such as Patient, Encounter, Observation, and MedicationRequest while preserving interoperability context, terminology consistency, and clinical workflow accuracy during modernization.
Common challenges include semantic mismatches, missing FHIR resource fields, terminology normalization complexity, custom Z-segment handling, API performance bottlenecks, backward compatibility issues, and interoperability governance gaps during phased healthcare modernization initiatives.
FHIR converter implementation uses transformation engines, middleware, APIs, and interoperability platforms to convert HL7 messages into FHIR resources while applying mapping logic, terminology normalization, validation rules, orchestration workflows, and real-time interoperability processing.
Artificial intelligence helps automate terminology mapping, detect transformation inconsistencies, identify semantic mismatches, monitor interoperability pipelines, validate synchronization accuracy, and improve large-scale healthcare data transformation workflows during HL7 to FHIR modernization initiatives.
Healthcare organizations validate readiness through schema testing, API reliability checks, interoperability simulations, US Core profile validation, synchronization monitoring, regression testing, and security verification to ensure production environments can support scalable and reliable healthcare interoperability workflows.
- On June 29, 2026
- 0 Comment

