Cloverleaf to FHIR Interface Engine Migration: Strategy Building Guide
Do you know about the Cloverleaf interface engine?
Well, you must have heard about it, and you might also have been using it, because it is a famous and widely adopted interface engine for connecting disparate systems. It still processes millions of HL7 messages every day.
However, in today’s modern healthcare interoperability, real-time APIs, cloud-based integration, and scalable data exchange with FHIR are used. And with the 21st Century Cures Act and TEFCA accelerating the shift towards an interoperable ecosystem, the Cloverleaf to FHIR migration is becoming essential.
Because the goal is not to eliminate HL7 v2 completely, but to modernize the system interoperability infrastructure to coexist with FHIR integration capabilities. But legacy interface engine modernization is not so simple as it has years of customization that need to be carefully handled to make it successful.
This is where a strong Cloverleaf to FHIR interface engine migration strategy that carefully plans phased migration, governance, testing, and operational continuity. And I think the reason you have landed on this blog is also for understanding how to migrate from Cloverleaf to modern interface engines without disrupting existing workflows.
So, in this guide, we will break down how to build a robust Cloverleaf to FHIR migration strategy for successful healthcare middleware replacement and moving legacy healthcare interfaces to FHIR-based architecture.
Why Healthcare Organizations Are Moving to FHIR-Based Interface Engines
Till now, the HL7 v2 messaging, along with batch-data exchange, has been enough to support healthcare workflows. The workflows were simple, moving from ADT to EHR and then to lab or pharmacy systems, simply connecting labs, pharmacies, and other healthcare systems.
However, modern healthcare is not limited to just connecting the healthcare systems. It also connects with patient-facing apps, third-party healthcare applications, and all these systems require real-time and scalable data exchange.
This is where traditional HL7 messages fall short, and integrating FHIR-based APIs becomes more than just essential; it becomes a strategic decision. And this is one of the biggest reasons why healthcare organizations are shifting to Cloverleaf FHIR integration and API-driven architecture.
With FHIR, healthcare organizations can easily exchange specific healthcare data without sharing entire patient records. Moreover, the APIs speed up the data exchange and make it easier, scalable, and flexible to integrate systems in the modern healthcare ecosystem.
Additionally, the modern healthcare interface engine also helps organizations to:
- Exchange data in real-time with APIs.
- Cloud-based integration and scalability.
- Event-driven interoperability workflows.
- Faster third-party integrations.
- Better API governance and security.
Another important reason why organizations are modernizing their interface engine is that Cloverleaf limits scalability. Because of the years of use, it accumulates custom Xlate logic, TPS scripts, and interface dependencies, which become too difficult to maintain.
Most importantly, the regulations such as the 21st Century Cures Act and TEFCA, are pushing organizations to accelerate the adoption of API-first interoperability. However, you don’t need to replace HL7 workflows, but to adopt a hybrid infrastructure that supports FHIR and modern interoperability needs at the same time.
Assessing Legacy Cloverleaf Environments
If you are modernizing Cloverleaf, then directly starting the process can quickly lead to failures if you don’t assess the interface engine carefully. Because, as said earlier, the Cloverleaf environments have evolved over the years and include multiple custom integrations, HL7 routines, and TPS scripts.
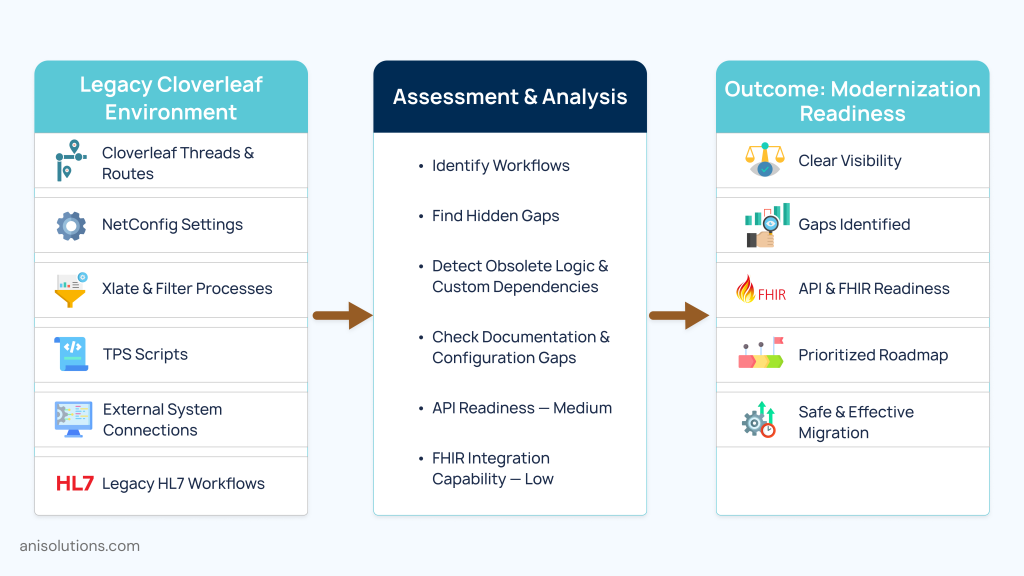
This is why, before starting the legacy interface engine modernization process, assessment is one of the most important steps. So, here is what you need to assess before healthcare middleware replacement:
- Cloverleaf threads and routes.
- NetConfig settings.
- Xlate and filter processes.
- TPS scripts.
- External system connections.
- Legacy HL7 workflows.
By assessing these components, you can identify the workflows and data pipelines that move data across systems in the daily operations. In this, you can understand multiple hidden gaps such as missing documentation, custom business logic that is obsolete, and many others.
One more important part of the assessment process is evaluating the API readiness and FHIR integration capabilities. Because Cloverleaf was not designed for RESTful APIs or resource-based data exchange. With this assessment, you can set priorities and understand which services must be updated first and which HL7 workflows can work temporarily.
This helps in planning the stages of modernization and building an effective Cloverleaf to FHIR migration strategy.
Building a Cloverleaf to FHIR Migration Strategy
Once you understand where your Cloverleaf interface engine stands, the next step is to build a migration strategy that will help modernize your system without disrupting existing workflows. And you need to avoid a common mistake of trying to replace everything at once.
Every successful migration is done in phases because suddenly shifting everything from the old to the new interface engine is not possible. Most importantly, you can’t just remove the HL7 v2 workflows as they run multiple clinical and operational processes.
That’s why adopting a hybrid approach is the best option, where the interoperability infrastructure depends on the HL7 while slowly integrating FHIR APIs. There are three approaches that you can choose from:
- Side-by-side migration where the Cloverleaf and modern healthcare interface engine run simultaneously, slowly shifting data and workflows to the new engine.
- Full interface engine replacement is shifting everything at once within a set time period.
- The hybrid coexistence model is where both HL7 and FHIR APIs work together and FHIR integration capabilities are integrated gradually over time.
Many healthcare organizations choose the third approach as it reduces operational risks and increases the success rate significantly. And even if there are some issues, you can quickly fall back to your old system, minimizing downtime.
Another important part is defining governance, security, and ensuring HIPAA compliance for the legacy interface engine modernization. By doing this, you can increase data safety and maintain data integrity without compromising quality and accuracy.
You also need to evaluate the integrations that need to be modernized first for better effectiveness. Because the end goal is not replacing Cloverleaf, it is building a scalable interoperability infrastructure that grows with your healthcare organization.
Executing a Cloverleaf to FHIR Migration
After building the Cloverleaf to FHIR migration strategy, the next step is to execute it in a way that does not compromise scalability and flexibility. However, doing so is not as simple as it seems, as the biggest challenge is the customization of interoperability environments from years of use.
The custom HL7 data transformations, Xlate processes, TPS scripts, and workflow dependencies are connected across multiple platforms. So, you can’t just copy and paste the workflows and patient data into the modern healthcare interface engine.
The most important step here is to identify which HL7 workflows should be converted into FHIR resources in the first phase. The systems, such as patient access applications, external healthcare APIs, and real-time interoperability services, must be transformed first.
But during this process, it is important to carefully map HL7 data structures into FHIR resources while maintaining interoperability continuity across existing systems. This means you need to standardize and normalize terminologies using standards such as:
- LOINC
- SNOMED CT
- RxNorm
Another reason why you need to carefully map the workflows is to maintain data integrity during transformation. Because even a small inconsistency can impact clinical workflows, reporting accuracy, or patient data accessibility.
Using AI-assisted mapping tools makes this whole process much easier and accurate, saving you time and resources. These tools can help you identify custom interface logic, automate schema discovery, recommend data mappings, and detect interoperability inconsistencies during transformation.
To ensure everything goes smoothly, you must continuously monitor interoperability performance throughout the modernization and migration process.
Testing, Validation, & Go-Live Readiness
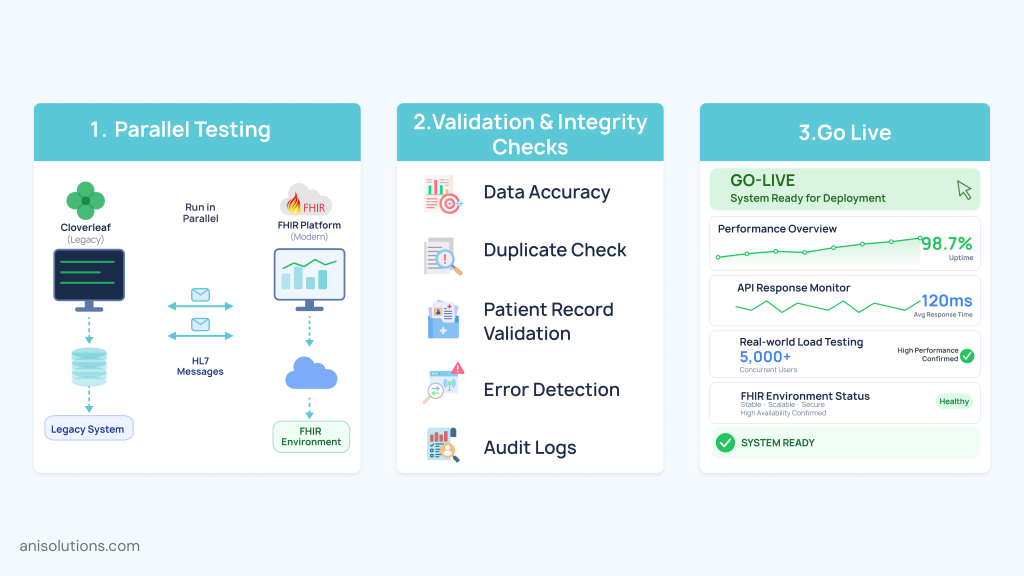
The final phase of the Cloverleaf to FHIR interface engine migration is testing whether or not the migration and modernization are working as they should. Without actual testing, confirming the success can lead to a collapse after it goes live.
That’s why you need to make sure that it can handle the real-world messaging load. But for this, you must run both systems in parallel to ensure that ongoing processes don’t get interrupted if the systems fail during the testing phase.
One more thing that you must confirm is the data validity and integrity of the migrated data. You need to check the data accuracy, potential duplication, and loss of some patient records. After confirming this, if there are any inconsistencies, you need to ensure they are fixed before going live.
Finally, after completing the modernization, you need to test the system under real-world message loads. This evaluates the performance of the systems along with the gaps that can create issues after going live.
If everything is working fine along with the API response rates, audit logging, and other components, then you can deploy the modernization without any worries.
Conclusion: Future-Proofing Healthcare Interoperability
In a nutshell, a modern healthcare organization needs to move beyond HL7 and Cloverleaf. However, to do so, you don’t have to completely replace the Cloverleaf interface engine, but just modernize it with FHIR integration capabilities.
With this, your healthcare organization can easily achieve real-time API-driven and scalable data exchange that modern healthcare interoperability requires. But you can’t replace everything at once; you need to modernize the systems phase-by-phase with robust governance, while maintaining operational continuity.
So, if your current interface engine is slowing down your practice, then it is time to modernize it. And A&I Solutions can help you do so without compromising compliance and security. Connect with our subject matter experts, and let’s assess your current interface engine.
Frequently Asked Questions
Healthcare organizations are prioritizing Cloverleaf to FHIR migration because modern interoperability now depends on APIs, cloud connectivity, patient-facing applications, and real-time data exchange that traditional HL7-centric integration environments struggle to support efficiently.
The biggest challenges include undocumented interfaces, custom TPS scripts, outdated HL7 workflows, hidden system dependencies, data mapping complexity, operational continuity risks, interoperability gaps, and maintaining clinical workflow stability during healthcare middleware replacement and modernization initiatives.
A modern healthcare interface engine improves interoperability by supporting FHIR APIs, real-time data exchange, cloud-native scalability, event-driven workflows, API governance, third-party integrations, and flexible interoperability management across connected healthcare systems and digital health platforms.
The best Cloverleaf to FHIR migration strategy is usually a phased hybrid approach where legacy HL7 workflows continue operating while FHIR APIs and modern interoperability services are introduced gradually to reduce downtime risks and maintain operational continuity.
Organizations migrate legacy healthcare interfaces by assessing existing workflows, mapping HL7 messages to FHIR resources, modernizing interoperability incrementally, maintaining hybrid coexistence environments, validating integrations continuously, and prioritizing high-impact APIs and interoperability services during phased migration.
Organizations protect protected health information (PHI) during migration through encryption, secure API access controls, audit logging, role-based permissions, continuous monitoring, secure testing environments, and compliance planning aligned with HIPAA requirements.
A Cloverleaf migration project timeline depends on interface complexity, customization levels, interoperability scope, and organizational size. Smaller migrations may take several months, while enterprise healthcare modernization initiatives can extend across multiple phases over one to two years.
Yes, many healthcare organizations use phased migration strategies, parallel interoperability environments, real-time synchronization, and hybrid HL7-FHIR coexistence models to modernize legacy Cloverleaf environments while minimizing downtime and maintaining uninterrupted clinical operations.
- On June 24, 2026
- 0 Comment